
In Vitro Antibacterial Activity of Ceftobiprole and Comparator Compounds against Nation-Wide Bloodstream Isolates and Different Sequence Types of MRSA

Abstract
:1. Introduction
2. Results
2.1. The Antibacterial Activity of Ceftobiprole and Comparator Compounds against Gram-Positive Bacteria
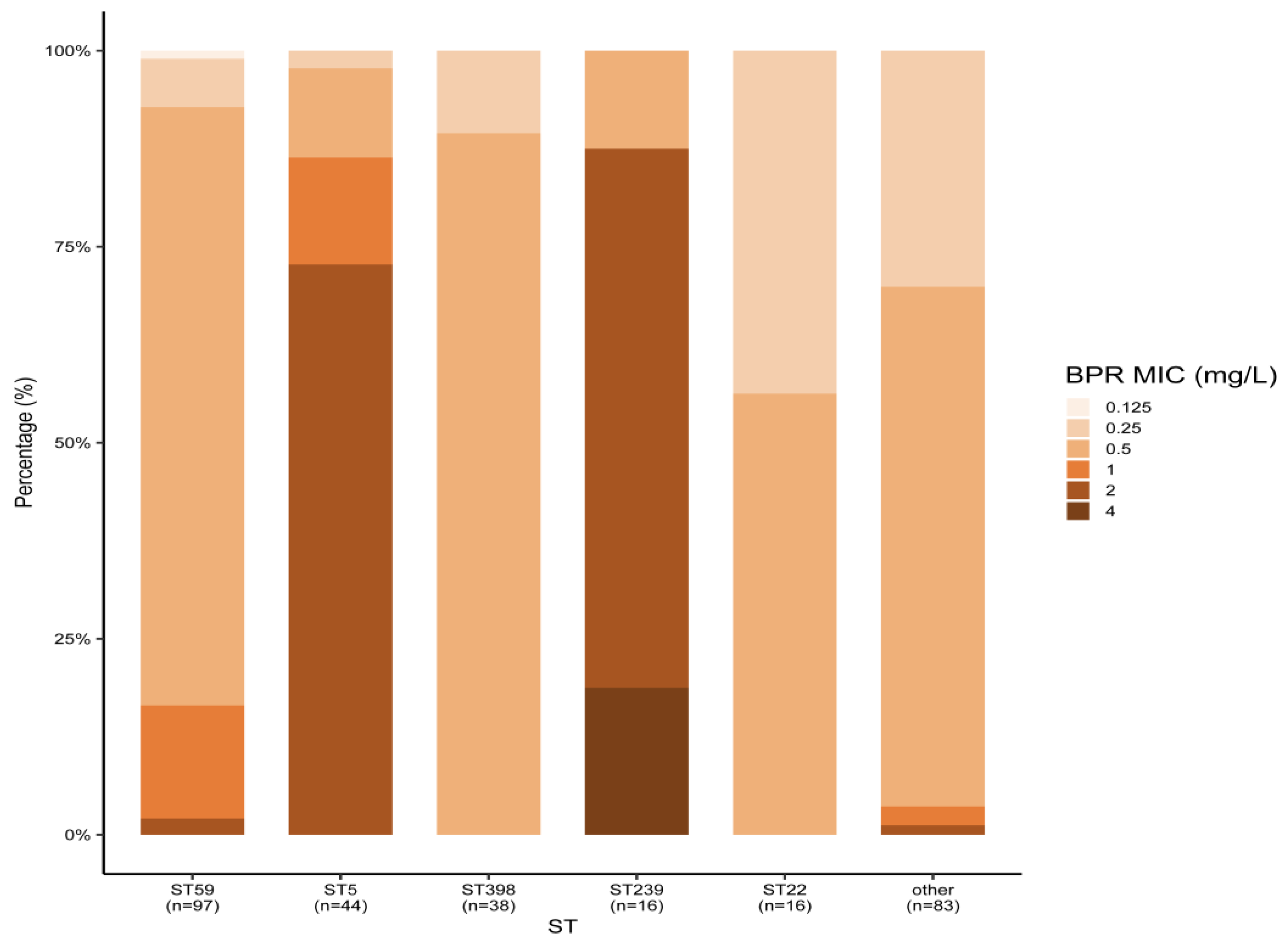
2.2. Sensitivity of Different Sequence Types of MRSA to Ceftobiprole and Comparator Compounds
2.3. The Antibacterial Activity of Ceftobiprole and Comparator Compounds against Gram-Negative Bacteria
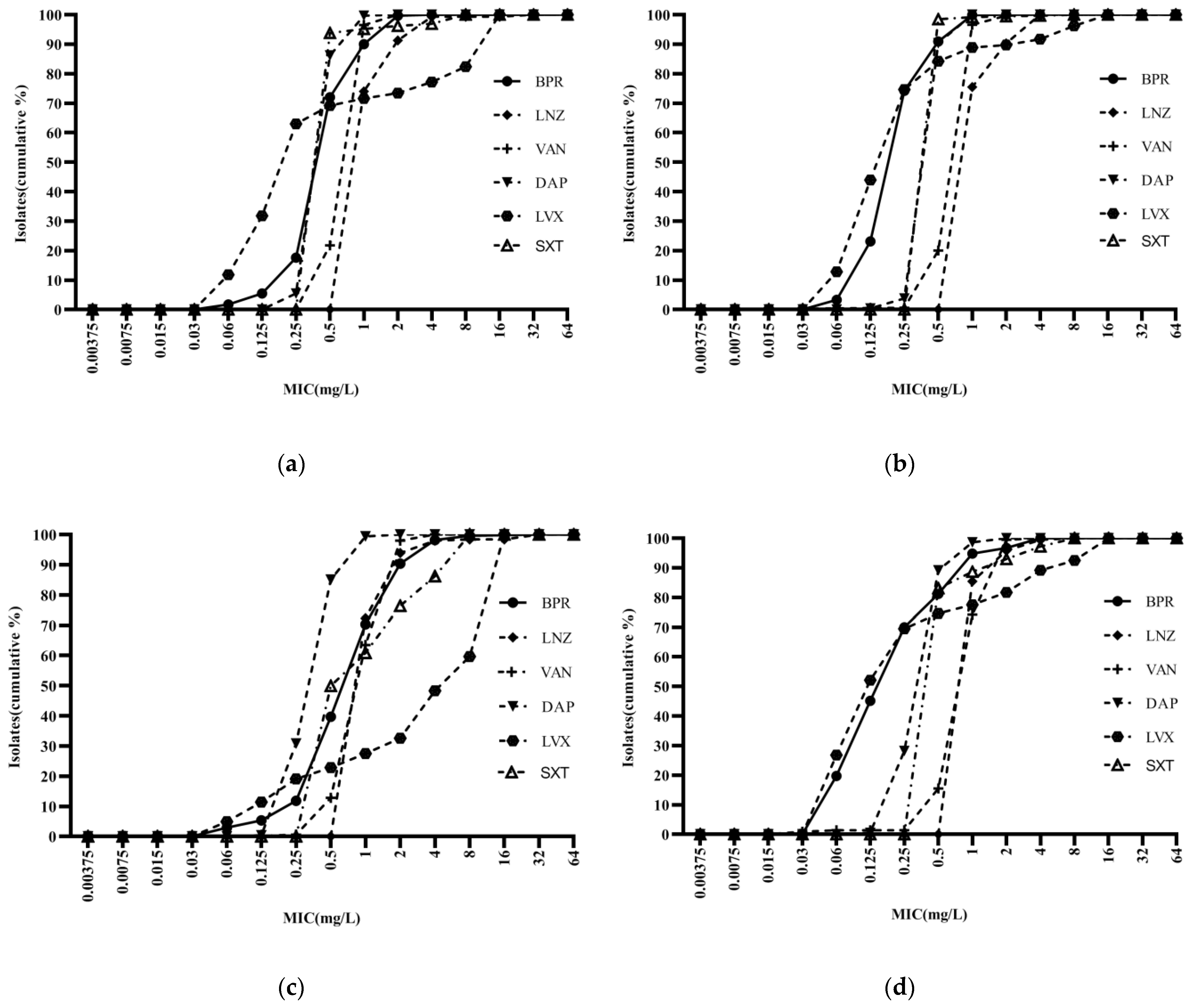
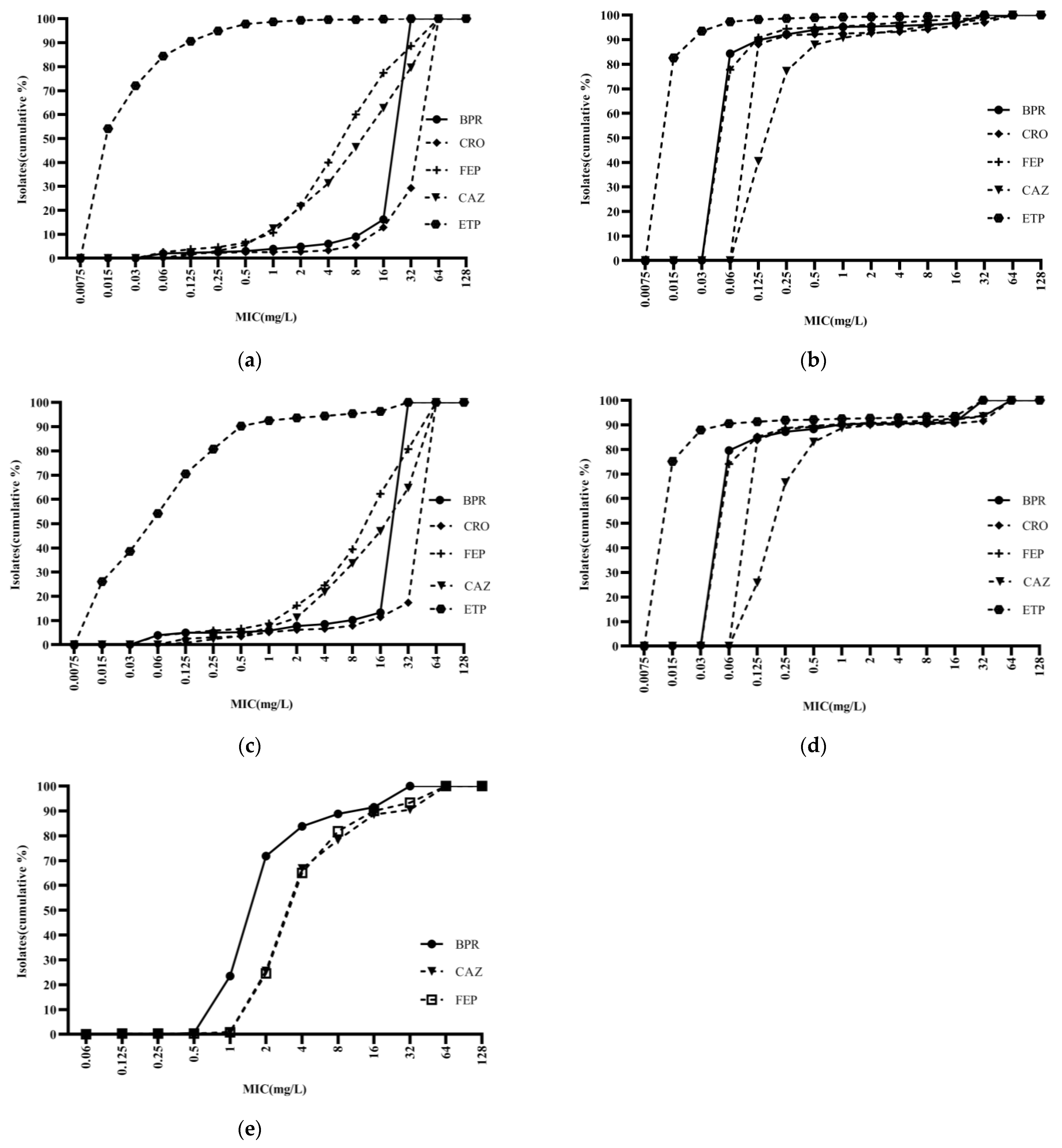
2.4. The Cumulative MIC Distribution of Ceftobiprole and Comparator Compounds against Major Bacteria
3. Discussion
4. Materials and Methods
4.1. Strain Sources
4.2. Antibiotics and Determination of Minimum Inhibitory Concentrations (MICs)
4.3. MRSA Sequence Typing
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention: Sepsis. Available online: https://www.cdc.gov/sepsis/what-is-sepsis.html (accessed on 11 February 2022).
- Xu, J.; Yuan, Y.; Wang, B.; Zhang, Q.; Wang, J.; Wang, S.; Li, Y.; Yan, W. Microbiological Analysis and Mortality Risk Factors in Patients with Polymicrobial Bloodstream Infections. Infect. Drug Resist. 2023, 16, 3917–3927. [Google Scholar] [CrossRef]
- GBD 2019 Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 2221–2248. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Report on the Epidemiology and Burden of Sepsis: Current Evidence, Identifying Gaps and Future Directions; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/334216 (accessed on 8 December 2021).
- Ohnuma, T.; Chihara, S.; Costin, B.; Treggiari, M.; Bartz, R.R.; Raghunathan, K.; Krishnamoorthy, V. Epidemiology, Resistance Profiles, and Outcomes of Bloodstream Infections in Community-Onset Sepsis in the United States. Crit. Care Med. 2023, 51, 1148–1158. [Google Scholar] [CrossRef] [PubMed]
- Rossolini, G.M.; Dryden, M.S.; Kozlov, R.S.; Quintana, A.; Flamm, R.K.; Läuffer, J.M.; Lee, E.; Morrissey, I.; on behalf of the CLASS Study Group; Fille, M.; et al. Comparative activity of ceftobiprole against Gram-positive and Gram-negative isolates from Europe and the Middle East: The CLASS study. J. Antimicrob. Chemother. 2011, 66, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Flamm, R.K.; Mendes, R.E.; Streit, J.M.; Smart, J.I.; Hamed, K.A.; Duncan, L.R.; Sader, H.S. Ceftobiprole Activity against Gram-Positive and -Negative Pathogens Collected from the United States in 2006 and 2016. Antimicrob. Agents Chemother. 2018, 63, e01566-18. [Google Scholar] [CrossRef] [PubMed]
- Duncan, L.R.; Hamed, K.A.; Smart, J.I.; Pfaller, M.A.; Flamm, R.K.; Mendes, R.E. Ceftobiprole activity against Gram-positive and Gram-negative pathogens causing bone and joint infections in the United States from 2016 to 2020. Diagn. Microbiol. Infect. Dis. 2022, 103, 115713. [Google Scholar] [CrossRef] [PubMed]
- Karlowsky, J.A.; Adam, H.J.; Decorby, M.R.; Lagacé-Wiens, P.R.; Hoban, D.J.; Zhanel, G.G. In vitro activity of ceftaroline against gram-positive and gram-negative pathogens isolated from patients in Canadian hospitals in 2009. Antimicrob. Agents Chemother. 2011, 55, 2837–2846. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Hawser, S.; Kothari, N.; Jemmely, N.; Redder, N. Susceptibility of ceftobiprole against Gram-positive and Gram-negative clinical isolates from 2019 from different European territories. J. Glob. Antimicrob. Resist. 2022, 29, 393–397. [Google Scholar] [CrossRef]
- Dandan, Y.; Shi, W.; Yang, Y.; Yonggui, Z.; Zhu, D.; Yan, G.; Hu, F. Antimicrobial activity of ceftobiprole and comparator agents when tested against gram-positive and -negative organisms collected across China (2016–2018). BMC Microbiol. 2022, 22, 282. [Google Scholar] [CrossRef]
- Amsler, K.M.; Davies, T.A.; Shang, W.; Jacobs, M.R.; Bush, K. In vitro activity of ceftobiprole against pathogens from two phase 3 clinical trials of complicated skin and skin structure infections. Antimicrob. Agents Chemother. 2008, 52, 3418–3423. [Google Scholar] [CrossRef] [PubMed]
- Holland, T.L.; Cosgrove, S.E.; Doernberg, S.B.; Jenkins, T.C.; Turner, N.A.; Boucher, H.W.; Pavlov, O.; Titov, I.; Kosulnykov, S.; Atanasov, B.; et al. Ceftobiprole for Treatment of Complicated Staphylococcus aureus Bacteremia. N. Engl. J. Med. 2023, 389, 1390–1401. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Zhuang, H.; Di, L.; Wang, Z.; Chen, Y.; Jiang, S.; Gu, C.; Sun, L.; Wang, H.; Zhu, Y.; et al. Staphylococcal cassette chromosome mec amplification as a mechanism for ceftobiprole resistance in clinical methicillin-resistant Staphylococcus aureus isolates. Clin. Microbiol. Infect. 2022, 28, 1151.e1–1151.e7. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Sun, S.; Yang, C.; Chen, H.; Yin, Y.; Li, H.; Zhao, C.; Wang, H. The Changing Pattern of Population Structure of Staphylococcus aureus from Bacteremia in China from 2013 to 2016: ST239-030-MRSA Replaced by ST59-t437. Front. Microbiol. 2018, 9, 332. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, Y.; Zhu, Y.; Dai, Y.; Hong, X.; Liu, Q.; Li, T.; Qin, J.; Ma, X.; Lu, H.; et al. Increased Community-Associated Infections Caused by Panton-Valentine Leukocidin-Negative MRSA, Shanghai, 2005-2014. Emerg. Infect. Dis. 2016, 22, 1988–1991. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Giani, T.; Coppi, M.; Di-Pilato, V.; Arena, F.; Colavecchio, O.L.; Conte, V.; Santerre-Henriksen, A.; Rossolini, G.M.; MRSA-HAP Study Group. Staphylococcus aureus from hospital-acquired pneumonia from an Italian nationwide survey: Activity of ceftobiprole and other anti-staphylococcal agents, and molecular epidemiology of methicillin-resistant isolates. J. Antimicrob. Chemother. 2019, 74, 3453–3461. [Google Scholar] [CrossRef] [PubMed]
- Hawser, S.; Kothari, N.; Karlowsky, J.A.; Wiktorowicz, T.; Hamed, K. In vitro susceptibility testing of ceftobiprole against 880 European respiratory tract infection isolates of methicillin-resistant Staphylococcus aureus followed by whole genome sequencing of ceftobiprole-resistant isolates. Diagn. Microbiol. Infect. Dis. 2020, 96, 114978. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Flamm, R.K.; Duncan, L.R.; Streit, J.M.; Castanheira, M.; Sader, H.S. Antimicrobial activity of ceftobiprole and comparator agents when tested against contemporary Gram-positive and -negative organisms collected from Europe (2015). Diagn. Microbiol. Infect. Dis. 2018, 91, 77–84. [Google Scholar] [CrossRef]
- Banerjee, R.; Gretes, M.; Basuino, L.; Strynadka, N.; Chambers, H.F. In vitro selection and characterization of ceftobiprole-resistant methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2008, 52, 2089–2096. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Lam, A.; Schweizer, F.; Thomson, K.; Walkty, A.; Rubinstein, E.; Gin, A.S.; Hoban, D.J.; Noreddin, A.M.; Karlowsky, J.A. Ceftobiprole: A review of a broad-spectrum and anti-MRSA cephalosporin. Am. J. Clin. Dermatol. 2008, 9, 245–254. [Google Scholar] [CrossRef]
- Hawser, S.; Kothari, N.; Jemmely, N.; Redder, N. Surveillance of ceftobiprole against Gram-positive and Gram-negative clinical isolates from 2018 from different European territories. J. Glob. Antimicrob. Resist. 2021, 26, 326–329. [Google Scholar] [CrossRef]
- Sader, H.S.; Castanheira, M.; Huband, M.D.; Shortridge, D.; Carvalhaes, C.G.; Mendes, R.M. Antimicrobial activity of dalbavancin against Gram-positive bacteria isolated from patients hospitalized with bloodstream infection in United States and European medical centers (2018–2020). Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ji, J.; Ying, C.; Liu, Z.; Yang, Q.; Kong, H.; Xiao, Y.; Blood Bacterial Resistant Investigation Collaborative System (BRICS) Study Group. Blood bacterial resistant investigation collaborative system (BRICS) report: A national surveillance in China from 2014 to 2019. Antimicrob. Resist. Infect. Control 2022, 11, 17. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Cormican, M.; Flamm, R.K.; Mendes, R.E.; Jones, R.N. Temporal and Geographic Variation in Antimicrobial Susceptibility and Resistance Patterns of Enterococci: Results From the SENTRY Antimicrobial Surveillance Program, 1997–2016. Open Forum Infect. Dis. 2019, 6, S54–S62. [Google Scholar] [CrossRef] [PubMed]
- Moon, T.M.; D’Andréa, É.D.; Lee, C.W.; Soares, A.; Jakoncic, J.; Desbonnet, C.; Garcia-Solache, M.; Rice, L.B.; Page, R.; Peti, W. The structures of penicillin-binding protein 4 (PBP4) and PBP5 from Enterococci provide structural insights into β-lactam resistance. J. Biol. Chem. 2018, 293, 18574–18584. [Google Scholar] [CrossRef] [PubMed]
- Lazzaro, L.M.; Cassisi, M.; Stefani, S.; Campanile, F. Impact of PBP4 Alterations on β-Lactam Resistance and Ceftobiprole Non-Susceptibility Among Enterococcus faecalis Clinical Isolates. Front. Cell. Infect. Microbiol. 2022, 11, 816657. [Google Scholar] [CrossRef] [PubMed]
- Henry, X.; Amoroso, A.; Coyette, J.; Joris, B. Interaction of ceftobiprole with the low-affinity PBP 5 of Enterococcus faecium. Antimicrob. Agents Chemother. 2010, 54, 953–955. [Google Scholar] [CrossRef] [PubMed]
- Buetti, N.; Marschall, J.; Timsit, J.F.; Atkinson, A.; Kronenberg, A.; Sommerstein, R.; Swiss Centre for Antibiotic Resistance (ANRESIS). Distribution of pathogens and antimicrobial resistance in bacteraemia according to hospitalization duration: A nationwide surveillance study in Switzerland. Clin. Microbiol. Infect. 2021, 27, 1820–1825. [Google Scholar] [CrossRef]
- Silva, N.; Radhouani, H.; Gonçalves, A.; Araújo, C.; Rodrigues, J.; Igrejas, G.; Poeta, P. In vitro activity of ceftobiprole against Gram-positive and Gram-negative bacteria isolated from humans and animals. J. Antimicrob. Chemother. 2010, 65, 801–803. [Google Scholar] [CrossRef]
- Hebeisen, P.; Heinze-Krauss, I.; Angehrn, P.; Hohl, P.; Page, M.G.; Then, R.L. In vitro and in vivo properties of Ro 63-9141, a novel broad-spectrum cephalosporin with activity against methicillin-resistant staphylococci. Antimicrob. Agents Chemother. 2001, 45, 825–836. [Google Scholar] [CrossRef]
- Hanson, N.D.; Sanders, C.C. Regulation of inducible AmpC beta-lactamase expression among Enterobacteriaceae. Curr. Pharm. Des. 1999, 5, 881–894. [Google Scholar] [CrossRef]
- Queenan, A.M.; Shang, W.; Kania, M.; Page, M.G.; Bush, K. Interactions of ceftobiprole with beta-lactamases from molecular classes A to D. Antimicrob. Agents Chemother. 2007, 51, 3089–3095. [Google Scholar] [CrossRef]
- Hancock, R.E. Resistance mechanisms in Pseudomonas aeruginosa and other nonfermentative gram-negative bacteria. Clin. Infect. Dis. 1998, 27 (Suppl. 1), S93–S99. [Google Scholar] [CrossRef] [PubMed]
- Jean, S.S.; Lee, W.S.; Yu, K.W.; Liao, C.H.; Hsu, C.W.; Chang, F.Y.; Ko, W.C.; Chen, R.J.; Wu, J.J.; Chen, Y.H.; et al. Rates of susceptibility of carbapenems, ceftobiprole, and colistin against clinically important bacteria collected from intensive care units in 2007: Results from the Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART). J. Microbiol. Immunol. Infect. 2016, 49, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Queenan, A.M.; Shang, W.; Bush, K.; Flamm, R.K. Differential selection of single-step AmpC or efflux mutants of Pseudomonas aeruginosa by using cefepime, ceftazidime, or ceftobiprole. Antimicrob. Agents Chemother. 2010, 54, 4092–4097. [Google Scholar] [CrossRef] [PubMed]
- Sakoulas, G.; Moellering, R.C.; Eliopoulos, G.M. Adaptation of methicillin-resistant Staphylococcus aureus in the face of vancomycin therapy. Clin. Infect. Dis. 2006, 42, S40–S50. [Google Scholar] [CrossRef] [PubMed]
- Wayne, P.A.; Clinical and Laboratory Standards Insitute. M100 Performance Standards for Antimicrobial Susceptibility Testing, 31st ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2021; pp. 70–73. [Google Scholar]
- Morroni, G.; Brenciani, A.; Brescini, L.; Fioriti, S.; Simoni, S.; Pocognoli, A.; Mingoia, M.; Giovanetti, E.; Barchiesi, F.; Giacomett, A.; et al. High Rate of Ceftobiprole Resistance among Clinical Methicillin-Resistant Staphylococcus aureus Isolates from a Hospital in Central Italy. Antimicrob. Agents Chemother. 2018, 62, e01663-18. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Agent | MIC (mg/L) 1 | R (%) 4 | S (%) 5 | ||
|---|---|---|---|---|---|
| MIC Range | MIC50 2 | MIC90 3 | |||
| Methicillin-resistant Staphylococcus aureus (MRSA) (289) | |||||
| Ceftobiprole | ≤0.06–4 | 0.5 | 1 | 0.4 | 99.6 |
| Linezolid | ≤1–32 | ≤1 | 2 | 0.7 | 99.3 |
| Daptomycin | 0.25–2 | 0.5 | 1 | / 6 | 99.6 |
| Vancomycin | 0.5–2 | 1 | 1 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5–>8 | ≤0.5 | ≤0.5 | 3.8 | 96.2 |
| Rifampicin | ≤0.00375–>8 | ≤0.00375 | ≤0.00375 | 1.4 | 97.6 |
| Levofloxacin | ≤0.06–>16 | 0.25 | 16 | 26.6 | 71.6 |
| Methicillin-susceptible Staphylococcus aureus (MSSA) (784) | |||||
| Ceftobiprole | ≤0.06–2 | 0.25 | 1 | 0 | 100.0 |
| Linezolid | ≤1–4 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | 0.25–1 | 0.5 | 0.5 | 0 | 100.0 |
| Vancomycin | ≤0.03–4 | 1 | 1 | 0 | 99.7 |
| Cotrimoxazole | ≤0.5–8 | ≤0.5 | ≤0.5 | 0.5 | 99.5 |
| Rifampicin | ≤0.00375–>8 | ≤0.00375 | ≤0.00375 | 0.5 | 99.4 |
| Levofloxacin | ≤0.06–>16 | 0.25 | 4 | 10.3 | 88.9 |
| Methicillin-resistant coagulase-negative Staphylococcus (MRCNS) (491) | |||||
| Ceftobiprole | ≤0.06–>32 | 1 | 2 | 9.6 | 90.4 |
| Linezolid | ≤1–>32 | ≤1 | 2 | 2.0 | 98.0 |
| Daptomycin | 0.125–2 | 0.5 | 1 | / | 99.4 |
| Vancomycin | ≤0.03–4 | 1 | 2 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5–>8 | ≤0.5 | 8 | 23.2 | 76.8 |
| Rifampicin | ≤0.00375–>8 | ≤0.00375 | 0.0075 | 8.4 | 91.6 |
| Levofloxacin | ≤0.06–>16 | 8 | 16 | 67.4 | 27.5 |
| Methicillin-susceptible coagulase-negative Staphylococcus (MSCNS) (213) | |||||
| Ceftobiprole | ≤0.06–4 | 0.25 | 1 | 3.3 | 96.7 |
| Linezolid | ≤1–4 | ≤1 | 2 | 0.5 | 99.5 |
| Daptomycin | 0.125–2 | 0.5 | 1 | / | 98.6 |
| Vancomycin | ≤0.03–4 | 1 | 2 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5–>8 | ≤0.5 | 2 | 7.0 | 93.0 |
| Rifampicin | ≤0.00375–8 | ≤0.00375 | ≤0.00375 | 1.4 | 98.6 |
| Levofloxacin | ≤0.06–>16 | 0.125 | 8 | 18.3 | 77.5 |
| Enterococcus faecium (397) | |||||
| Ceftobiprole | 0.125–>32 | >32 | >32 | - 7 | - |
| Tigecycline | ≤0.06–2 | 0.125 | 0.125 | - | 98.5 |
| Daptomycin | ≤0.06–>8 | 1 | 2 | 0.5 | 99.5 |
| Vancomycin | 0.5–>4 | 1 | 1 | 0 | 100.0 |
| Linezolid | ≤1–>4 | ≤1 | 2 | 0 | 98.2 |
| Teicoplanin | ≤0.125–>2 | 0.5 | 0.5 | 0 | 100.0 |
| Levofloxacin | 0.25–>16 | 16 | >16 | 80.9 | 16.9 |
| Rifampicin | 0.25–>8 | 4 | 8 | 77.3 | 11.8 |
| Ciprofloxacin | ≤0.125–>16 | 16 | >16 | 88.7 | 9.1 |
| Erythromycin | ≤1–>32 | 32 | >32 | 80.9 | 9.1 |
| Penicillin G | ≤1–>32 | >32 | >32 | 83.1 | 16.9 |
| Enterococcus faecalis (296) | |||||
| Ceftobiprole | 0.125–>32 | 0.25 | 2 | - | - |
| Tigecycline | ≤0.06–0.25 | 0.125 | 0.125 | 0 | 100.0 |
| Daptomycin | ≤0.06–>8 | 1 | 2 | 0.7 | 92.9 |
| Vancomycin | ≤0.25–>2 | 1 | 2 | 0 | 100.0 |
| Linezolid | ≤1–>4 | 1 | 2 | 0 | 95.3 |
| Teicoplanin | ≤0.125–>2 | 0.5 | 0.5 | 0 | 100.0 |
| Levofloxacin | 0.25–>16 | 1 | 16 | 31.4 | 68.2 |
| Rifampicin | 0.25–>8 | 2 | 8 | 49.0 | 25.0 |
| Ciprofloxacin | ≤0.125–>16 | 1 | >16 | 32.1 | 64.5 |
| Erythromycin | ≤1–>32 | 32 | >32 | 57.1 | 32.1 |
| Penicillin G | ≤1–>32 | 2 | 32 | 13.5 | 86.5 |
| Agent | MIC (mg/L) 1 | R (%) 4 | S (%) 5 | ||
|---|---|---|---|---|---|
| MIC Range | MIC50 2 | MIC90 3 | |||
| ST59 (97) | |||||
| Ceftobiprole | 0.125–2 | 0.5 | 1 | 0 | 100.0 |
| Linezolid | ≤1–2 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | ≤0.06–1 | 0.5 | 1 | 0 | 100.0 |
| Vancomycin | 0.125–4 | 1 | 1 | 0 | 99.0 |
| Cotrimoxazole | ≤0.5 | ≤0.5 | ≤0.5 | 0 | 100.0 |
| Rifampicin | ≤0.00375–>8 | ≤0.00375 | 0.0075 | 3.1 | 96.9 |
| Levofloxacin | ≤0.06–>16 | 0.125 | 4 | 11.3 | 88.7 |
| ST5 (44) | |||||
| Ceftobiprole | 0.25–2 | 2 | 2 | 0 | 100.0 |
| Linezolid | ≤1–2 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | ≤0.06–1 | 0.25 | 1 | 0 | 100.0 |
| Vancomycin | 0.25–2 | 0.5 | 1 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5 | ≤0.5 | ≤0.5 | 0 | 100.0 |
| Rifampicin | ≤0.00375–0.015 | ≤0.00375 | 0.0075 | 0 | 100.0 |
| Levofloxacin | 0.125–>16 | 16 | >16 | 84.1 | 15.9 |
| ST398 (38) | |||||
| Ceftobiprole | 0.25–0.5 | 0.5 | 0.5 | 0 | 100.0 |
| Linezolid | ≤1–2 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | ≤0.06–1 | 0.25 | 1 | 0 | 100.0 |
| Vancomycin | 0.5–2 | 0.5 | 1 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5–2 | ≤0.5 | ≤0.5 | 0 | 100.0 |
| Rifampicin | ≤0.00375–0.015 | ≤0.00375 | 0.0075 | 0 | 100.0 |
| Levofloxacin | 0.125–8 | 0.25 | 0.5 | 2.6 | 97.4 |
| ST239 (16) | |||||
| Ceftobiprole | 0.5–4 | 2 | 4 | 18.8 | 81.2 |
| Linezolid | ≤1–2 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | 0.125–1 | 0.5 | 0.5 | 0 | 100.0 |
| Vancomycin | 0.5–2 | 0.5 | 2 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5–8 | ≤0.5 | 8 | 18.8 | 81.2 |
| Rifampicin | ≤0.00375–>8 | 8 | >8 | 56.3 | 43.7 |
| Levofloxacin | 0.125–>16 | 16 | >16 | 87.5 | 12.5 |
| ST22 (16) | |||||
| Ceftobiprole | 0.25–0.5 | 0.5 | 0.5 | 0 | 100.0 |
| Linezolid | ≤1–2 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | 0.25–1 | 0.5 | 1 | 0 | 100.0 |
| Vancomycin | 0.25–1 | 0.5 | 1 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5 | ≤0.5 | ≤0.5 | 0 | 100.0 |
| Rifampicin | ≤0.00375–0.0075 | ≤0.00375 | 0.0075 | 0 | 100.0 |
| Levofloxacin | ≤0.06–0.5 | 0.125 | 0.25 | 0 | 100.0 |
| Other (83) | |||||
| Ceftobiprole | 0.25–2 | 0.5 | 0.5 | 0 | 100.0 |
| Linezolid | ≤1–2 | ≤1 | 2 | 0 | 100.0 |
| Daptomycin | 0.125–1 | 0.5 | 1 | 0 | 100.0 |
| Vancomycin | 0.25–2 | 0.5 | 1 | 0 | 100.0 |
| Cotrimoxazole | ≤0.5–1 | ≤0.5 | ≤0.5 | 0 | 100.0 |
| Rifampicin | ≤0.00375–>8 | ≤0.00375 | 0.015 | 1.2 | 96.4 |
| Levofloxacin | ≤0.06–16 | 0.25 | 8 | 14.5 | 85.5 |
| Agent | MIC (mg/L) 1 | R (%) 4 | S (%) 5 | ||
|---|---|---|---|---|---|
| MIC Range | MIC50 2 | MIC90 3 | |||
| Escherichia coli (ESBL−) (2050) | |||||
| Ceftobiprole | ≤0.03–>32 | 0.06 | 0.25 | 7.9 | 92.1 |
| Ceftazidime | ≤0.125–>64 | 0.25 | 1 | 4.5 | 93.8 |
| Ceftriaxone | ≤0.125–>64 | ≤0.125 | 0.25 | 7.2 | 92.5 |
| Cefepime | ≤0.06–>64 | ≤0.06 | 0.125 | 2.2 | 96.1 |
| Ertapenem | ≤0.015–>32 | ≤0.015 | 0.03 | 0.8 | 99.2 |
| Escherichia coli (ESBL+) (2035) | |||||
| Ceftobiprole | ≤0.06–>32 | 32 | >32 | 97.4 | 2.6 |
| Ceftazidime | ≤0.125–>64 | 16 | 64 | 53.5 | 31.3 |
| Ceftriaxone | ≤0.125–>64 | 64 | >64 | 97.3 | 2.6 |
| Cefepime | ≤0.06–>128 | 8 | 64 | 40.0 | 15.5 |
| Ertapenem | ≤0.015–>32 | ≤0.015 | 0.125 | 1.3 | 97.8 |
| Klebsiella pneumoniae (ESBL−) (1404) | |||||
| Ceftobiprole | ≤0.06–>32 | ≤0.06 | 1 | 12.8 | 87.2 |
| Ceftazidime | ≤0.125–>64 | 0.25 | 4 | 9.0 | 90.4 |
| Ceftriaxone | ≤0.125–>64 | ≤0.125 | 2 | 10.0 | 89.7 |
| Cefepime | ≤0.06–>64 | ≤0.06 | 1 | 8.3 | 90.8 |
| Ertapenem | ≤0.015–>32 | ≤0.015 | 0.06 | 7.5 | 92.1 |
| Klebsiella pneumoniae (ESBL+) (482) | |||||
| Ceftobiprole | ≤0.06–>32 | 32 | >32 | 95.0 | 5.0 |
| Ceftazidime | ≤0.125–>64 | 32 | >64 | 66.4 | 21.8 |
| Ceftriaxone | ≤0.125–>64 | 64 | >64 | 93.8 | 5.2 |
| Cefepime | ≤0.06–>128 | 16 | 64 | 60.6 | 16.2 |
| Ertapenem | ≤0.015–>32 | 0.06 | 0.5 | 5.6 | 90.0 |
| Enterobacter aerogenes (ESBL−) (97) | |||||
| Ceftobiprole | ≤0.06–>32 | ≤0.06 | 0.125 | 4.1 | 95.9 |
| Ceftazidime | ≤0.125–>64 | 0.5 | 64 | 20.6 | 75.3 |
| Ceftriaxone | ≤0.125–>64 | ≤0.125 | 32 | 26.8 | 70.1 |
| Cefepime | ≤0.06–>64 | ≤0.06 | 0.5 | 1.0 | 98.0 |
| Ertapenem | ≤0.015–4 | 0.03 | 0.5 | 1.0 | 96.9 |
| Enterobacter aerogenes (ESBL+) (14) | |||||
| Ceftobiprole | ≤0.06–>32 | 32 | >32 | 78.6 | 21.4 |
| Ceftazidime | ≤1–>64 | 32 | >64 | 85.7 | 14.3 |
| Ceftriaxone | ≤1–>64 | 64 | >64 | 92.9 | 7.1 |
| Cefepime | ≤0.06–64 | 4 | 64 | 50.0 | 42.9 |
| Ertapenem | ≤0.015–>32 | 0.25 | 1 | 7.1 | 85.7 |
| Klebsiella oxytoca (ESBL−) (91) | |||||
| Ceftobiprole | ≤0.06–>32 | 0.25 | 32 | 36.3 | 63.7 |
| Ceftazidime | ≤0.125–32 | ≤0.125 | 0.5 | 1.0 | 97.8 |
| Ceftriaxone | ≤0.125–16 | ≤0.125 | 1 | 6.6 | 90.1 |
| Cefepime | ≤0.06–64 | ≤0.06 | 0.5 | 1.0 | 97.8 |
| Ertapenem | ≤0.015–>32 | ≤0.015 | 0.03 | 2.2 | 96.7 |
| Klebsiella oxytoca (ESBL+) (11) | |||||
| Ceftobiprole | 32–>32 | 32 | >32 | 100.0 | 0 |
| Ceftazidime | 0.5–>64 | 16 | >64 | 54.5 | 27.3 |
| Ceftriaxone | 32–>64 | 64 | >64 | 100.0 | 0 |
| Cefepime | ≤0.06–>64 | 8 | 32 | 36.4 | 9.0 |
| Ertapenem | ≤0.015–8 | 0.06 | 2 | 18.2 | 81.8 |
| Enterobacter cloacae (273) | |||||
| Ceftobiprole | ≤0.06–>32 | ≤0.06 | 32 | 26.0 | 74.0 |
| Ceftazidime | ≤0.125–>64 | 0.5 | 64 | 23.1 | 72.9 |
| Ceftriaxone | ≤0.125–>64 | 0.25 | 64 | 26.4 | 69.6 |
| Cefepime | ≤0.06–>64 | ≤0.06 | 16 | 11.4 | 81.3 |
| Ertapenem | ≤0.015–>32 | ≤0.015 | 1 | 8.1 | 89.0 |
| Salmonella spp. (125) | |||||
| Ceftobiprole | ≤0.06–>32 | ≤0.06 | 8 | 10.4 | 88.8 |
| Ceftazidime | ≤0.125–>64 | ≤0.125 | 1 | 6.4 | 92.8 |
| Ceftriaxone | ≤0.125–>64 | ≤0.125 | 16 | 5.6 | 88.2 |
| Cefepime | ≤0.06–>64 | ≤0.06 | 0.5 | 4.0 | 93.6 |
| Ertapenem | ≤0.015–0.125 | ≤0.015 | ≤0.015 | 0 | 100.0 |
| Serratia marcescens (100) | |||||
| Ceftobiprole | ≤0.06–>32 | 0.125 | 8 | 14.0 | 86.0 |
| Ceftazidime | ≤0.125–>64 | 0.5 | 8 | 6.0 | 91.0 |
| Ceftriaxone | ≤0.125–>64 | 0.25 | 16 | 8.0 | 88.0 |
| Cefepime | ≤0.06–64 | 0.125 | 2 | 4.0 | 93.0 |
| Ertapenem | ≤0.015–4 | ≤0.015 | 0.25 | 5.0 | 93.0 |
| Pseudomonas aeruginosa (400) | |||||
| Ceftobiprole | 0.5–>32 | 2 | 16 | - 6 | - |
| Ceftazidime | 1–>64 | 4 | 32 | 11.5 | 78.3 |
| Cefepime | 0.125–>64 | 4 | 16 | 10.0 | 81.8 |
| Acinetobacter baumannii (308) | |||||
| Ceftobiprole | ≤0.06–>32 | 32 | >32 | - | - |
| Ceftazidime | ≤0.125–>64 | 64 | >64 | 61.4 | 37.0 |
| Cefepime | ≤0.06–>64 | 64 | >64 | 63.3 | 35.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Zhou, W.; Chen, Y.; Shen, P.; Xiao, Y. In Vitro Antibacterial Activity of Ceftobiprole and Comparator Compounds against Nation-Wide Bloodstream Isolates and Different Sequence Types of MRSA. Antibiotics 2024, 13, 165. https://doi.org/10.3390/antibiotics13020165
Li L, Zhou W, Chen Y, Shen P, Xiao Y. In Vitro Antibacterial Activity of Ceftobiprole and Comparator Compounds against Nation-Wide Bloodstream Isolates and Different Sequence Types of MRSA. Antibiotics. 2024; 13(2):165. https://doi.org/10.3390/antibiotics13020165
Chicago/Turabian StyleLi, Lingqin, Wangxiao Zhou, Yunbo Chen, Ping Shen, and Yonghong Xiao. 2024. "In Vitro Antibacterial Activity of Ceftobiprole and Comparator Compounds against Nation-Wide Bloodstream Isolates and Different Sequence Types of MRSA" Antibiotics 13, no. 2: 165. https://doi.org/10.3390/antibiotics13020165